The Cognitive Health Market Cannot Be Built on Jobs Alone

Authored on
Modified
Dementia is a market problem, not just a medical one Work may help, but it is not a cure Prevention must start before crisis

Dementia is now a market-structure issue, not just a medical one. Nearly 57 million people globally had dementia in 2021 and the annual global cost was already projected to be US$1.3 trillion in 2019. That sum does not stay solely within hospital walls. It spills into homes, unpaid work, lost productivity, pensions, insurance policies and local economies. This creates the need of clearer framework for the cognitive health market. The simple version of the narrative says that maintaining employment may support the brain. The more complex narrative is that work is a poor stand-in for a healthcare infrastructure. It may provide routine, meaningful activity, social interaction and cognitive challenge. But these may be accompanied by stress, injury, shift work, inadequate wages and marginalization. A serious healthcare market, then, must not promote work as a panacea for the aging mind, but consider which systems can detect risk early, reduce family strain and keep older adults functioning before decline becomes a crisis.
The cognitive health market is already larger than memory care
The first policy mistake is to regard cognitive decline as a subsidiary of neurology clinics. The bulk of the cost occurs long before anyone is diagnosed with dementia. Families experience it, employers notice errors, a series of small slips at home and in work build up, but junior GPs have little time to assemble the cues. Then the market reacts. It buys scans, care beds, home help, medicines and crisis services, long after the measure of risk is fixed. That is a costly infrastructure. It favors rescue over prevention. And it obscures the real consumer. It is not merely the patient. It is the spouse, who watches hours of work slip away, the insurer who subsidizes rising claims and the tax-funded health system that covers for the private sector's shortfall.
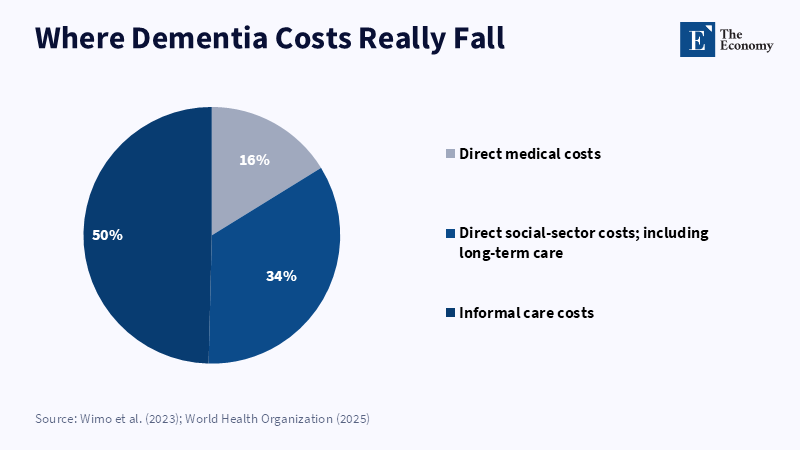
This matters because dementia costs are already too high for a late-care model. A 2025 US estimate calculated the total annual cost of dementia, including medical care, long-term care, unpaid care, lost earnings and lost quality of life, at US$781 billion. It is not a small clinical market. It is a whole economy of decline. The same estimate calculated the medical and long-term care costs at US$232 billion. But family and friends delivered 6.8 billion hours worth of care, valued at US$233 billion. These stark figures tell us that a cognitive health market cannot be judged simply by new drug pipelines or care-home capacity. It must be judged on the extent to which it postpones need, preserves family output and avoids preventable attrition.
The conventional discussion of later-life employment is useful, but too thin. Employment may be linked to cognitive health, but the channel matters. Is the possible benefit coming from income, social contact, daily routine, mental challenge, physical movement, identity, access to care, or lower stress? Each answer points to a different healthcare market. If income is the channel, wage support and pension design matter. If social contact is the channel, community care matters. If mental demand is the channel, job quality and adult learning matter. A market that cannot separate these channels will reward slogans and underfund prevention.
Employment is a poor indicator of brain shielding
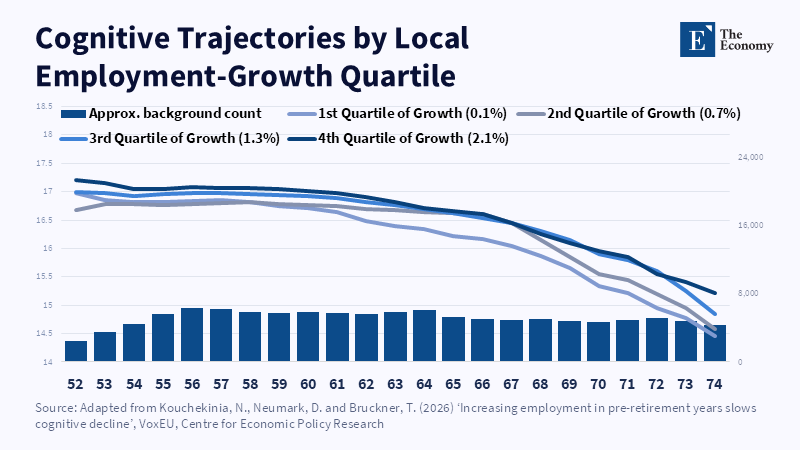
The strongest recent claims about work and cognition should be interpreted differently. Using evidence from local labor-demand shocks to show weaker employment among older men years and worse later cognitive scores. One summary found using the estimates that a 10-point increase in national unemployment (a rise in the unemployment rate of about 1 percentage point in good states) reduced log-cognitive scores on average by about 0.11 to 0.19. That is not trivial. But it is not robust for women, for people over 65, or for workers in types not experiencing location-responsive labor demand shifts in the same manner. The result suggests a severe message. It does not indicate that a given job can guard any brain.
Would this difference affect market structure? A man leaving a factory town aged 58 is not the same as a professional opting for part-time at 66 (or, for that matter, a lowly-paid warehouse worker can be employed and still have pain, poor sleep, stress and little cognitive challenge). A night-shifting nurse is not the same as a consultant with control over time. A retiree can have left work and still maintain a strong social life, getting involved in voluntary work, getting regular exercise and mentally active hobbies. Employment status is easy to measure, but a blunt indicator. It may conflate attachment with stimulation and stimulation with security.
Better evidence pushes us away from the simple question of whether people work and towards the better question of what work is like. A 2024 study of more than 7,000 Norwegians found that less cognitively demanding jobs in adulthood were associated with a heightened risk of mild cognitive impairment and dementia after age 70. The comparison is significant because it recasts the issue from employment as an either/or to the kind of work people do. Jobs that entail monotonous routines and low mental demand may not foster the same reserve as jobs that require the use of judgment, social give-and-take, planning and learning. The policy lesson is not keep everyone working. It is "don't let midlife turn into a long period of low control, low learning, high stress employment."
Prevention should be established before retirement
The cognitive health market has a timing issue. It invests heavily when decline is already visible, but does too little during the years in which risk accumulates. A 2024 Lancet Commission suggested that around 45% of dementia cases worldwide could be postponed or avoided through intervention on 14 modifiable risk factors over the life course. The list is neither exotic nor multidimensional. It includes hearing impairment, hypertension, diabetes, smoking, depression, social disengagement, physical inactivity, air pollution, elevated low-density lipoprotein and untreated visual impairment. Paid work will likely influence some of these factors. It is possible to reduce disengagement and support income. But this is likely to increase stress, sleep disturbance, injuries and access inequalities. That is precisely why paid work cannot be the main form of primary prevention.
Better markets would be in late middle age, not late disease. They would see the 50s and early 60s as a prevention window. Primary-care packages would monitor blood pressure, cholesterol, diabetes, hearing, vision, depression, sleep and memory complaints in one joined pathway. This is also where remote monitoring can support prevention before decline becomes visible. Employers would be assessed on age-friendly job design, not retirement benefits alone. Insurers would pay for prevention that keeps older adults stable, not just crisis care. Local governments would track where older workers are leaving the labor market because the local economy has hollowed out. That data wouldn't authenticate brain decline. It would highlight places where financial strain, lost routine and health risk may coalesce.
It also avoids a cruel moral trap. Telling people to keep on working to keep their brains intact can become a kind, if indirect, way of blaming aging bodies for their collapse. It can also become a back door to raising retirement ages, without upgrading working life in the process. This would be a misguided policy. The aim is not to force a weary body to serve the labor market for a longer time. The aim is to make later working life safer, more adaptable and more valuable wherever work is an option and people still want it. Where the option is not available, the cognitive input must be delivered outside work by setting up community projects and scheduled volunteering, retraining schemes, exercise classes and social prescribing.
The logic of these disparities reveals why this cannot be left to the discretion of the individual. In 2024, the average employment rate among workers 55–64 was just 64.6% throughout the OECD, compared to 80.1% among workers 25–54; for workers 60–64, the rate was approximately 55.9%, with enormous variation across nations. Skill gaps are widening the divide. In 55–64 year-olds, the rate of employment among those with tertiary education was substantially higher than it was for those with upper-secondary education or less. Consequently, those most likely to exit employment early are stuck the most, with fewer buffers to health shocks. An equitable market for cognitive health would do away with that divide, not applaud employment in the abstract.
Healthcare rankings need to gauge brain-age preparedness
Market signals must shift. The healthcare industry already rates hospitals, insurers, care providers and local systems on many measures of quality. Brain-age readiness should be one of them. The same logic should apply across clinical fields, where prevention and early detection shape long-term market quality. A practical ranking would not ask, Which provider mentions dementia most often. Instead, it would ask, Which system detects risk early, links the medical and social safety net, lowers preventable caregiver strain and keeps midlife adults stable and independent before they are high-cost patients. This would clarify the cognitive health market. At that point, brain-age readiness becomes a system-redesign issue, not just a medical service issue. It would also incentivize providers who embed prevention into everyday care, rather than leaving families to navigate the system after a crisis.
The indicators must be usable. One batch might evaluate approaches to early diagnosis: pathways to memory loss complaints, follow-up with general practitioners, hearing and sight assessments, management of depression and optimal management of vascular risk factors. A second set might approve of various forms of market access: waiting times insurance cover, co-payment regimes andreach into remote country districts and ethnic groups. A third group of indicators might provide such support in the community that precedes or complements clinical care: training of family carers, access to temporary out-of-home care, social activity clubs, employment and vocational advice and employer contacts. A fourth batch might evaluate age-friendly adjustments to the workplace and elderly people's transitional phases: graduated retirement, the systematic re-design of work tasks, easier work shifts and the retraining of displaced older employees. This would not turn the priority-setting into an attractive cross-country beauty contest. It would rather reveal a disparate set of services into a tangible market framework.
Some critics might say this requires health systems to address labor-market problems. That's a legitimate but limited criticism: healthcare already pays for the costs of labor-market failures-stress-related disease, disabilities, delayed diagnosis, collapse of caregivers-and it also gains when prevention is successful. Some say that cognitive outcomes are the wrong length of time to measure: too slow. This criticism has some merit. However, intermediate measures can be drawn for risk factors listed above and then systems would not need to wait years for an endpoint (a dementia diagnosis).
A darker critique is that prevention markets may merely be another form of selection. The rich will buy better screening, better jobs, cleaner places, more support and the poor will get a slogan about resilience. That is precisely why measures and market design matter. Without defined metrics, the cognitive health market will reward branding. With defined measures, the market can identify gaps. It will reveal which systems protect only the well-to-do and which treat high-need groups. It will prove whether employers and providers are shouldering some of the burden or whether costs are falling on families.
The opening statistic must set the agenda. A condition that costs the world over $1 trillion per year can’t be managed simply as a private memory problem or left solely to clinics. Work may, under some circumstances and through some pathways, benefit some brains. This warrants research, but it is an insufficient policy. The challenge now is to develop a cognitive health market where work is one input, not the output. The market must internalize and incentivize prevention, work quality, early diagnosis and care. Yet the new frontier of healthcare competition must be clear, not who offers the best late-stage response, but who preserves human functioning longer.
The views expressed in this article are those of the author(s) and do not necessarily reflect the official position of The Economy or its affiliates.
References
Edwin, T.H., Håberg, A.K., Zotcheva, E., Bratsberg, B., Jugessur, A., Engdahl, B., Bowen, C., Selbæk, G., Kohler, H.P., Harris, J.R., Tom, S.E., Krokstad, S., Mekonnen, T., Stern, Y., Skirbekk, V.F. and Strand, B.H. (2024) ‘Trajectories of occupational cognitive demands and risk of mild cognitive impairment and dementia in later life: The HUNT4 70+ Study’, Neurology, 102(9), e209353.
Kouchekinia, N.A., Neumark, D. and Bruckner, T.A. (2026) ‘Does employment slow cognitive decline? Evidence from labor market shocks’, NBER Working Paper No. 35117, National Bureau of Economic Research.
Kouchekinia, N.A., Neumark, D. and Bruckner, T.A. (2026) ‘Increasing employment in pre-retirement years slows cognitive decline’, VoxEU, Centre for Economic Policy Research.
Livingston, G., Huntley, J., Liu, K.Y., Costafreda, S.G., Selbæk, G., Alladi, S., Ames, D., Banerjee, S., Burns, A., Brayne, C., Fox, N.C., Ferri, C.P., Gitlin, L.N., Howard, R., Kales, H.C., Kivimäki, M., Larson, E.B., Nakasujja, N., Rockwood, K., Samus, Q., Shirai, K., Singh-Manoux, A., Schneider, L.S., Walsh, S., Yao, Y., Sommerlad, A. and Mukadam, N. (2024) ‘Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission’, The Lancet, 404(10452), pp. 572–628.
OECD (2025) OECD Employment Outlook 2025: Can We Get Through the Demographic Crunch? Paris: OECD Publishing.
Thorson, G. (2026) ‘Can employment protect older adults from cognitive decline?’, The Policy Scientist, 26 May.
United States Cost of Dementia Research Team (2025) The Cost of Dementia in 2025. Los Angeles: USC Schaeffer Center for Health Policy & Economics.
Wimo, A., Seeher, K., Cataldi, R., Cyhlarova, E., Dielemann, J.L., Frisell, O., Guerchet, M., Jönsson, L., Malaha, A.K., Nichols, E., Pedroza, P., Prince, M., Knapp, M. and Dua, T. (2023) ‘The worldwide costs of dementia in 2019’, Alzheimer’s & Dementia, 19(7), pp. 2865–2873.
World Health Organization (2025) ‘Dementia’, WHO Fact Sheet, 31 March.
Similar Post